Description
Discussion
MAG-O3® Patented Lipid Absorption Enhancement Technology (PLATform)
The MAG-O3® PLATform is a novel monoglyceride delivery system that enhances absorption of lipidbased
and lipid-soluble nutraceutical and food ingredients. This technology has been applied to The
Pharmacist Formula’s Omega Optima formula in order to create a unique vehicle by which to deliver EPA
and DHA. Due to the fact that monoglyceride oils are intrinsically emulsifiers and are, by nature, in a
readily absorbable form, they can bypass the body’s normal fat digestion process. These qualities make
Omega Optima an excellent method for delivering omega-3 fatty acids, especially to individuals with
digestive, pancreatic, or gall bladder challenges. Studies show that MAG-O3® fish oils (FO) have three
times (300%) greater absorption of EPA and DHA compared to other leading fish oils.
Quality
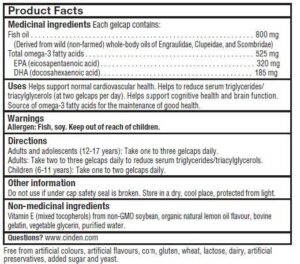
Omega Optima is made using proprietary MAG-O3® compositions containing monoglyceride FO with no
additional ingredients, carriers, or excipients. Every batch of fish oil ensure the world’s highest standards
for purity, potency, and freshness. The fish oil is non-GMO, certified sustainable and antibiotic-free.
Additionally, it is eco-friendly because the greater absorption of EPA and DHA ultimately means that fewer
grams of fish oil need to be harvested for the same benefit.
In Vitro and In Vivo Animal Studies
The ability of MAG-O3® -enhanced EPA and DHA to positively influence growth inhibition and apoptosis in
colorectal, breast, lung, and prostate diseased cell lines was first demonstrated in a series of in vitro studies.[4-6]
Researchers subsequently set out to demonstrate efficacy in animal models after oral administration. In three
separate animal models, MAG-O3® EPA and DHA forms showed superior activity on diseased cell-line growth
inhibition and cytokine production when compared to control, corn oil, krill oil, or the parent forms ethyl ester
(EE) EPA and ethyl ester (EE) DHA.[4,7,8] These in vivo animal studies proved that orally supplemented MAGO3
® EPA and DHA were well-absorbed and bioactive. Researchers postulated that the observed superior
effects of MAG-O3® EPA and DHA forms were the result of enhanced absorption, and they set out to prove this
hypothesis.
Preclinical Bioavailability Studies
The in vivo pharmacokinetic studies in rodents involved a comparison between MAG-O3® and its parent EE
DHA FO and an analysis of blood concentrations of DHA over time. The doses used were equivalent to human
doses of 3 g/day and 30 g/day; the latter was included primarily to investigate toxicity at high doses.
Researchers found that MAG-O3® DHA FO had a three times (3x) higher peak concentration, a 3x higher
saturation potential at the high dose, and a 3x higher absorption rate (at a 3 g/day equivalent human dose) than
its parent DHA FO. No toxicity was observed at either dose level.[1,2] This research demonstrated superior
bioavailability and presumably better exposure of cells to DHA.
Clinical Bioavailability Study
A phase 1, double-blind, randomized, crossover, pharmacokinetic study was performed in 20 healthy adults
aged between 19 and 71 years who were administered 6 g (containing 1800 mg EPA and 1200 mg DHA) per
day of EE FO or MAG-O3® .[3] Parameters studied were plasma EPA and DHA concentration (as percent of
total fatty acids), Cmax, and AUC. Compared to EE EPA+DHA, the results indicated that at peak
concentration, MAG-O3® EPA and DHA forms were 3x higher, they reached maximum concentration faster,
and maintained their plasma levels longer. The finding in the animal study was validated: the MAG-O3®
instantaneous absorption was 3x greater than the EE form. Likewise, the AUC over 24 hours was also more
than 3x higher (P<.0001) for MAG-O3® EPA and DHA (MAG-O3® FO).*
Not only did this study confirm the bioavailability findings in the animal study, but it also demonstrated that after
24 hours, the MAG-O3® maintained 2-3x higher blood levels of EPA and DHA than the EE FO. This means
that, given a daily dose, circulating EPA and DHA levels can be expected to ramp up over time and remain high
with steadily increasing exposure of cells to EPA, DHA, and their metabolites. Based on the results of the
bioavailability studies, an individual would get more EPA and DHA from MAG-O3® than from EE FO gram for
gram. Furthermore, as shown in the animal studies, one could anticipate enhanced effects. It is noteworthy that
all 20 adults who completed the study saw their omega-3 absorption enhanced when taking MAG-O3® .
Expanding Research
In vitro and animal studies have demonstrated the positive effects of MAG-O3® on airway immune response
(e.g., IgE, leukocytes); the expression of COX-2, NF-kB, cytokines (e.g., IL-6, IL-8), MUC5AC, and mucin; and
Ca(2+) hypersensitivity in lung tissues.[8-11] In other research, rats subjected to eight weeks of a high-fat, highcarbohydrate
diet were either not supplemented or provided 3 g/day of MAG-O3® DHA. Compared to the data
from the non-supplemented group, the data from the MAG-O3® DHA supplemented group clearly showed a
positive impact on cardiovascular health parameters. Measures included blood pressure, heart rate, serum
lipid levels, cytokine production, aortic wall thickness, and a DHA:AA ratio in aortic tissue, which correlated with
the production of resolvin D2 and D3 metabolites.*[12]
A Note About Resolvins and Other EPA and DHA Metabolites
Specialized proresolving lipid mediators, such as resolvins, protectins, and maresins, are EPA and DHA
metabolites naturally produced in vivo through enzymatic conversion of EPA and DHA. These mediators aid
the body’s “clean-up” response to the arachidonic acid cascade.[13] Rather than supplying a single molecule or
metabolite, which would mirror the pharmaceutical model, Omega Optima fish oils provide all the benefits of
EPA and DHA as well as the expected and desirable benefits of their metabolites.*

References
1. Unpublished, internal data. Ingenutra.
2. Fortin S, inventor; Centre de Recherche sur les Biotechnologies Marines, assignee. Compositions comprising polyunsaturated fatty acid monoglycerides or
derivatives thereof and uses thereof. US patent 8,198,324. June 12, 2012.
3. MaxSimil Patented Lipid Absorption Technology Clinical Study Report: MaxSimil® 3020 Omega-3. Sherbrooke (Québec), Canada: Ingenutra; 2015. [Unpublished,
internal data]
4. Morin C, Rousseau É, Fortin S. Anti-proliferative effects of a new docosapentaenoic acid monoacylglyceride in colorectal carcinoma cells. Prostaglandins Leukot
Essent Fatty Acids. 2013 Sep;89(4):203-13. [PMID: 23932824]
5. Fortin S, inventor; Centre de Recherche sur les Biotechnologies Marines, assignee. Polyunsaturated fatty acid monoglycerides, derivatives, and uses thereof. US
patent 8,119,690. February 21, 2012.
6. Fortin S, inventor; Centre de Recherche sur les Biotechnologies Marines, assignee. Polyunsaturated fatty acid monoglycerides, derivatives, and uses thereof. US
patent 8,329,747. December 11, 2012.
7. Morin C, Blier PU, Fortin S. Eicosapentaenoic acid and docosapentaenoic acid monoglycerides are more potent than docosahexaenoic acid monoglyceride to
resolve inflammation in a rheumatoid arthritis model. Arthritis Res Ther. 2015 May 29;17:142. [PMID: 26022389]
8. Morin C, Fortin S, Cantin AM, et al. Docosahexaenoic acid derivative prevents inflammation and hyperreactivity in lung: implication of PKC-Potentiated inhibitory
protein for heterotrimeric myosin light chain phosphatase of 17 kD in asthma. Am J Respir Cell Mol Biol. 2011 Aug;45(2):366-75. [PMID: 21057106]
9. Morin C, Fortin S, Cantin AM, et al. MAG-EPA resolves lung inflammation in an allergic model of asthma. Clin Exp Allergy. 2013 Sep;43(9):1071-82. [PMID:
23957343]
10. Morin C, Cantin AM, Rousseau É, et al. Pro-resolving action of MAG-DHA in lung inflammatory models related to cystic fibrosis. Am J Respir Cell Mol Biol. 2015
Oct;53(4):574-83. [PMID: 25781052]
11. Morin C, Fortin S, Rousseau É. New omega-3 derivatives reduce airway inflammation and prevent rho-kinase activation in an allergic model of asthma. J Aller
Ther. 2012;3(S1):003. doi:10.4172/2155-6121.S1-003.
12. Morin C, Rousseau E, Blier PU, et al. Effect of docosahexaenoic acid monoacylglyceride on systemic hypertension and cardiovascular dysfunction. Am J Physiol
Heart Circ Physiol. 2015 Jul 1;309(1):H93-H102. [PMID: 25910811]
13. Weylandt KH, Chiu CY, Gomolka B, et al. Omega-3 fatty acids and their lipid mediators: towards an understanding of resolvin and protectin formation.
Prostaglandins Other Lipid Mediat. 2012 Mar;97(3-4):73-82. [PMID: 22326554]
14. Guasch-Ferré M, Hu FB, Martínez-González MA, et al. Primary prevention of cardiovascular disease with a Mediterranean diet. N Engl J Med. 2013 Apr
4;368(14):1279-90. [PMID: 23432189]
15. Mayor S. Mediterranean diet reduces cardiovascular events in people with heart disease, study shows. BMJ. 2016 Apr 24;353:i2348. [PMID: 27114468]
16. Chiva-Blanch G, Badimon L, Estruch R. Latest evidence of the effects of the Mediterranean diet in prevention of cardiovascular disease. Curr Atheroscler Rep.
2014 Oct;16(10):446. [PMID: 25115436]
17. Fitó M, Cladellas M, de la Torre R, et al. Anti-inflammatory effect of virgin olive oil in stable coronary disease patients: a randomized, crossover, controlled trial.
Eur J Clin Nutr. 2008 Apr;62(4):570-74. [PMID: 17375118]
18. Ruano J, López-Miranda J, de la Torre R, et al. Intake of phenol-rich virgin olive oil improves the postprandial prothrombotic profile in hypercholesterolemic
patients. Am J Clin Nutr. 2007 Aug;86(2):341-46. [PMID: 17684203]
19. Gimeno E, de la Torre-Carbot K, Lamuela-Raventós RM, et al. Changes in the phenolic content of low density lipoprotein after olive oil consumption in men. A
randomized crossover controlled trial. Br J Nutr. 2007 Dec;98(6):1243-50. [PMID: 17617938]
20. Bogani P, Galli C, Villa M, et al. Postprandial anti-inflammatory and antioxidant effects of extra virgin olive oil. Atherosclerosis. 2007 Jan;190(1):181-86. [PMID:
16488419]
21. Guasch-Ferré M, Hu FB, Martínez-González MA, et al. Olive oil intake and risk of cardiovascular disease and mortality in the PREDIMED Study. BMC Med. 2014
May 13;12:78. [PMID: 24886626]
22. Castañer O, Covas MI, Khymenets O, et al. Protection of LDL from oxidation by olive oil polyphenols is associated with a downregulation of CD40-ligand
expression and its downstream products in vivo in humans. Am J Clin Nutr. 2012 May;95(5):1238-44. [PMID: 22440854]
23. Raederstorff D. Antioxidant activity of olive polyphenols in humans: a review. Int J Vitam Nutr Res. 2009 May;79(3):152-65. [PMID: 20209466]

Reviews
There are no reviews yet.